(The buccopharyngeal and cloacal membranes lack a mesodermal core, and thus fail to develop a blood supply - this might explain their later breakdown.)
The other layers of the digestive tract - for example: the muscular wall - are developed from splanchnic mesoderm. Similarly, organs such as the liver and pancreas arise as endodermal outgrowths from the gut tube, but mesoderm contributes to their development. (Recall that when the lateral mesoderm was split by the intra-embryonic coelom, one layer remained in association with the ectoderm - the somatic mesoderm, and one layer remained in contact with the endoderm - the splanchnic mesoderm.)
Contribution from the neural crest ...
Migrating into the splanchnic mesoderm of the developing digestive system will be many neural crest cells - these will play an important part in establishing the autonomic nerve supply to the gut. Can you think of an abnormality of the digestive system where this process of innervation has failed - usually in the distal portion of the large intestine? (clue: look up Hirschsprung's disease.)
The first important step in development of the digestive system occurs during folding of the embryonic disc as neurulation takes place (weeks 4 and 5) - the thin endodermal layer is ‘gathered up' inside the embryonic body to form a tubular structure.
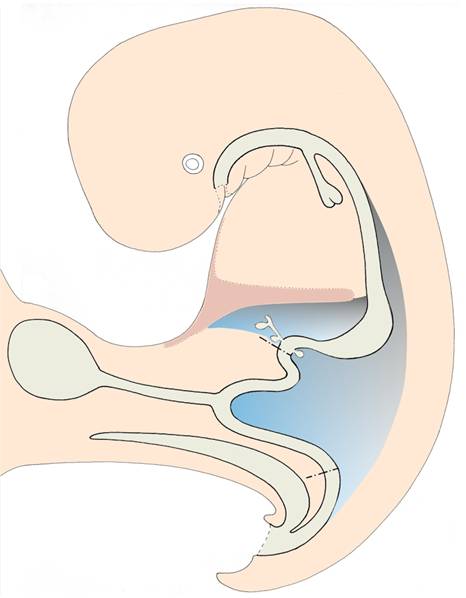
Gut tube, respiratory diverticulum, yolk sac, and allantois.

The vitelline duct
The endoderm of the original embryonic disc is continuous laterally with the endoderm enclosing the yolk sac. This continuity is retained throughout folding of the embryonic disc and for several weeks after this. Gradually, the connection between the embryo and the yolk sac becomes narrower, and a tubular vitelline duct is formed. Normally, the vitelline duct disappears completely by the end of the embryonic period, but an abnormal remnant may persist - for example: as a small diverticulum attached to the small intestine (Meckel's diverticulum), or a vitelline cyst or fistula.
The allantois
The allantois first appears as an endodermal outgrowth from the last part of the gut tube. It grows into the connecting stalk (which later becomes the umbilical cord) and gains a coating of mesodermal cells. The umbilical blood vessels develop within this mesoderm alongside the allantois, linking the embryo with the developing placenta. In many species, particularly the egg-layers, the allantois is an essential storage organ for nitrogenous wastes - for example urid acid - which are generated during embryonic development, but in the human embryo this role is unlikely, since nitrogenous wastes can be transferred across the placental membrane into the maternal blood stream. Most of the human embryonic allantois eventually regresses, but the proximal portion probably contributes to the apical region of the urinary bladder. If this process of regression fails, cystic remnants or even fistula linking the bladder with the umbilicus may be seen: urachal cyst or fistula.
Foregut, midgut, and hindgut
It is usual and helpful to subdivide the embryonic gut tube into three portions:
The blood supply and nerve supply to different regions of the digestive system reflect these subdivisions.
In the early embryo (ie: during the 4th and 5th weeks) it is difficult to be exact about the extent of each of these three regions, but as development proceeds, the distinctions become clearer.
List the different parts of the digestive system derived from the foregut, midgut, & hindgut.
Liver
The liver begins its development as a small endodermal outgrowth - the hepatic diverticulum - which arises from the caudal part of the foregut. This tubular outgrowth extends through the ventral mesentery into the septum transversum, branching as it grows. One branch is formed close to the septum transversum, and this subsequently develops into the gall bladder and cystic duct. The remaining branches are formed within the septum, and the mesodermal cells which surround this branching tubular system assist in the formation of the liver tissue. Thus, the endodermal hepatic diverticulum forms the duct system and storage organ of the biliary system, while the mesodermal cells contributed by the septum transversum form the liver cells.
The pancreas
This first appears as two endodermal buds which grow from the most caudal part of the foregut. There is a ventral pancreatic bud close to the origin of the hepatic diverticulum, and slightly larger dorsal pancreatic bud on the opposite side of the same region of the gut tube. These two buds will later come together and fuse to form the pancreas.
Mesenteries
Postnatally, the stomach, the jejunum and ileum, and some parts of the large intestine are supported from the posterior wall of the abdomen by membranous structures called mesenteries. It is through these mesenteries that blood vessels, lymph vessels, and nerves are distributed to and from the gut wall. The mesenteries allow mobility to the gut - an important aid to digestive processes. In the adult, the mesenteries have a complex arrangement, but this can be understood by working through the embryological processes which produce them.
In the embryo, the mesenteries have a much simpler organisation. There is a dorsal mesentery extending from the oesophagus to the hindgut, linking the gut tube to the posterior wall of the embryo. There is a less-extensive ventral mesentery from the ventral border of the stomach to the caudal surface of the septum transversum and the anterior abdominal wall. This originally simple arrangement is modified by a succession of changes in the position of the gut tube - bendings and rotations - which inevitably affect the mesenteries.
Competition for space
After its formation, the gut tube grows rapidly in length and bulk. But the abdominal portions of this system are competing for space in the relatively underdeveloped abdominal cavity with other rapidly growing organs, particularly the liver and the mesonephros (intermediate kidney).
As the liver grows, it bulges out from the caudal surface of the septum transversum and extends into the ventral mesentery, dividing this into two parts. The portion of the ventral mesentery between the stomach and the liver becomes the lesser omentum, while the portion between the liver and the anterior abdominal wall becomes the falciform ligament. (Recall that the umbilical vein is supported within the falciform ligament close to its free border, and channels blood into the ductus venosus which bypasses the liver sinusoids.)
The mesonephros is a transient set of structures contributing to the development of the urinary system. By the sixth week of development, the two mesonephric ridges form prominent bulges - one on each side of the dorsal mesentery - and they encroach upon the limited space available in the abdominal cavity.
Response of the gut tube
The abdominal portion of the gut tube, supported by its mesenteries, is relatively mobile, and during the next six weeks undergoes several significant changes in position and arrangement. Some of these changes are in response to the lack of space in the abdominal cavity; others result from inter-relationships with neighbouring structures:
1 the stomach bends and rotates
2 the duodenum swings across to the right side
3 the midgut loop herniates into the umbilical cord
4 the midgut returns to the abdominal cavity, rotating 270°
5 the mesenteries become modified by these positional changes
6 the hindgut is delimited by the urorectal septum.
1 the stomach bends and rotates
As the stomach develops, the dorsal border grows more rapidly than the ventral border. This differential growth causes the stomach to bend, and produces the greater and lesser curvatures.
At the same time, the stomach rotates through about 90°, so that the original left side comes to face ventrally, while the right side faces dorsally. Note the effect this rotation has on the vagus nerves supplying the stomach - the left vagus nerve supplies the future anterior surface of the stomach, the right vagus nerve the posterior surface.
2 the duodenum swings across to the right side
As the stomach rotates, the next part of the digestive tract - the duodenum - is carried with it, and forms a loop to the right side of the midline. The duodenum subsequently becomes ‘stuck down', or retroperitoneal in position.
This change in position of the duodenum also affects the position of the common bile duct and brings the two pancreatic buds together so that they can fuse. Before they fuse, each pancreatic bud develops its own duct system opening independently into the duodenum. After fusion, it is usual for the duct systems to link up and drain into the duodenum via the duct of the smaller ventral bud. The proximal portion of the duct in the dorsal bud may be retained as an accessory pancreatic duct. The spleen develops in the dorsal mesentery alongside the stomach.
3 the midgut loop herniates into the umbilical cord
The midgut loop grows rapidly in length at the same time that the liver and mesonephros are growing rapidly. In week 6 the midgut herniates into the proximal part of the umbilical cord - it enters a part of the extra-embryonic coelom that lies within the cord and is in continuity with the abdominal portion of the intra-embryonic coelom. The midgut continues its development in this herniated position until week 12, by which time there is sufficient room for it to return into the abdominal cavity. (By this time, the abdominal cavity has grown in size, the liver is growing less rapidly, and the mesonephros has regressed.)
Since this herniation is a part of normal development, it is sometimes referred to as ‘physiological herniation'.
4 the midgut returns to the abdominal cavity, rotating 270°
While it is herniated, and as it returns to the abdominal cavity, the midgut rotates about the axis of the superior mesenteric artery which supplies it. It rotates through a total of 270° in an anticlockwise direction (when viewed from the ventral aspect), although this rotation is completed only after the gut has returned to the abdominal cavity. It is this rotation and return of the midgut that arranges the digestive tract into the pattern seen postnatally.
5 the mesenteries become modified by these positional changes
Rotation of the stomach affects both dorsal and ventral mesenteries. The portion of the dorsal mesentery related to the stomach bulges out to the left to form the bag-like greater omentum, which eventually will lie in front of the transverse colon. The lesser omentum shifts from its sagittal position until it lies across the midline, from the lesser curvature of the stomach on the left to the liver on the right.
The dorsal mesentery related to the midgut loop becomes elongated and then twisted by the herniation and rotation of the midgut. After return of the midgut to the abdominal cavity, some parts of the mesentery become adherent to the posterior abdominal wall and are then resorbed, so that portions of the gut become retroperitoneal, like the duodenum.
6 the hindgut is delimited by the urorectal septum
Compared with other parts of the gut, the hindgut has a fairly straightforward development. The main event is formation of the urorectal septum - a wedge-shaped bar of mesoderm which lies at the junction of the allantois with the hindgut. The urorectal septum grows caudally until it contacts the cloacal membrane, subdividing it into two parts: the urogenital menbrane and the anal membrane. Thus, the hindgut is now completely separated from the urogenital system. (The urogenital and anal membranes perforate later, as noted in the previous section.)
Recanalisation
It may come as a surprise to learn that for a while during normal development, some parts of the central lumen of the gut tube become obliterated by proliferation of the cells in the epithelial lining. Later, this obstructing core becomes vacuolated and then disperses, so that the gut become recanalised. Errors in this process can produce many types of abnormalities: obstruction, narrowing, or duplication.
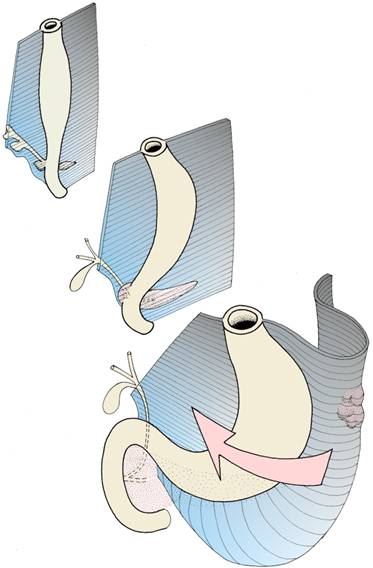
Stomach rotation - effect on the dorsal and ventral mesenteries
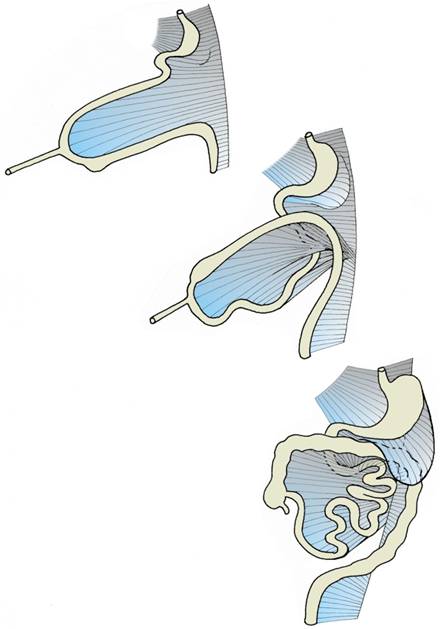
Rotation of the midgut
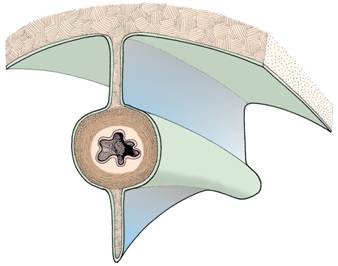
Dorsal and ventral mesenteries
Digestion begins before birth
The amniotic fluid swallowed by the fetus contains cells and debris shed from its skin. These are acted on by digestive juices and the products absorbed, but of course the baby's nutrition still comes via the placenta.
Abnormal development of the digestive system
Given such a complex developmental history, many abnormalities of the digestive system are possible. The most important categories are listed below:
Questions on development of the digestive system:
1 From which germ layers do the following develop:
a) the epithelial lining of most of the gut tube
b) the smooth muscle of the gut wall
c) the visceral and parietal peritoneum
d) the lining of the second half of the anal canal?
2 What is a mesentery? What is the extent of the
dorsal mesentery
ventral mesentery
in a 5-week embryo?
3 Which artery is associated with the embryonic midgut and its derivatives? Which arteries supply the developing duodenum?
4 Describe the allantois. Does it have a function in the human embryo?
5 What is the embryological explanation of Meckel's diverticulum? What might be some of the clinical complications of this abnormality?
6 Describe the early stages in development of the liver. Does development of the liver have any effect on the veins passing through the septum transversum as they return blood to the heart?
7 Which structures in the mouth are derived from the stomodeum?
8 Do neural crest cells contribute to development of the digestive system?
9 What factors are thought to cause physiological herniation of the midgut loop?
10 Which part of the herniated midgut loop returns to the abdominal cavity first?
11 Give an embryological explanation of why the left vagus nerve innervates the anterior wall of the stomach.
12 How is the main pancreatic duct formed?
13 What is an annular pancreas?
14 What effect does rotation and return of the midgut have on the dorsal mesentery?
15 Which structures are linked by the vitelline duct?
16 What is meant by imperforate anus? Give an embryological explanation of this condition.
17 Which artery supplies the hindgut and its derivatives? From which source do hindgut derivatives receive their parasympathetic nerve supply?
