These swellings consist of aggregations of mesodermal cells covered with ectoderm. Shallow grooves separate adjacent swellings.
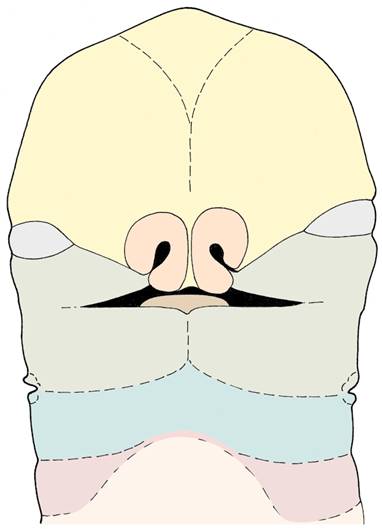
Note the proportions of the face early in development - the laterally-placed eyes, the wide mouth, and the low-set ears. We should not forget the important influence that structures such as the eyes, the tongue, the brain, the skull base, and the ear have on facial development: a defect in one of these structures can have a profound effect on facial development.
Recall the significant part played by the first pharyngeal arches in development of the face. A cartilage develops within the mandibular process - Meckel's cartilage - but (surprisingly) most of the mandible develops by intramembranous ossification around the outer surface of the cartilage. (Note that most of the facial skeleton is formed by intramembranous ossification.)
nose and nasal cavities
The first indication of nasal development is the formation of a pair of olfactory placodes on the frontonasal process. These invaginate and establish the nasal cavities which eventually open into the oral cavity. At the same time, mesodermal proliferation at the edges of each placode produces a C-shaped ridge. The two limbs of the ridge are known as the medial nasal swelling and the lateral nasal swelling. Note that initially the two halves of the nose are widely spaced - they move closer and fuse as development proceeds. (The eyes also move closer together.)
the grooves between the building blocks
Note carefully the grooves between the components of the developing face - several of these have a significance in normal and abnormal development.
In the groove between the maxillary process and the frontonasal process (including the lateral nasal swelling) the nasolacrimal duct develops by invagination of the surface ectoderm. (This duct links the conjuctival sac of the eye with the nasal cavity.)
The groove between the maxillary swelling and the medial nasal swelling is soon ‘smoothed out' as cells from the maxillary swelling stream medially. (It appears that the streams of cells from the left and right maxillary swellings eventually meet in the midline of the face, forming the upper lip.)
The midline groove between the two mandibular swellings is also soon filled out, but a midline junction between the two halves of the mandible persists for longer.
Don't forget that the muscles of facial expression are contributed by the second pharyngeal arch - the myoblasts have to migrate into the facial region.
Building blocks of the face
facial clefts
If the grooves between adjacent mesodermal swellings fail to fill out normally as the face develops, facial clefts arise. Cleft upper lip is the most common form, and is usually not exactly in the midline but slightly to one side, or sometimes bilateral. Consult your textbook and study carefully the different forms of cleft lip, and the consequences and treatment of these conditions. Read also about oblique facial clefts. In each case, try and relate these abnormalities to what you know about normal development of the face.
the palate
Many everyday activities depend on the presence of a normal palate - for example: chewing, swallowing, speaking. A cleft in this structure can have serious consequences for a baby.
There has been a lot of recent research into palatal closure, and we have a clearer idea now of the mechanisms at work. For example, it is now clear that the movement of the palatal shelves from a vertical to a horizontal position (so that they can fuse) is a rapid process, taking less than 1 second in rat embryos. An important prerequisite for this event is movement of the tongue downwards out of the way - this occurs when the embryo begins swallowing actions. Another fairly recent realisation is that neural crest cells play a vital role in palatal development, as they do in facial development generally.
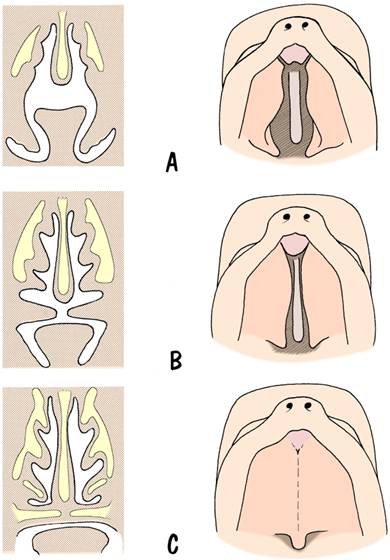
Development of the palate

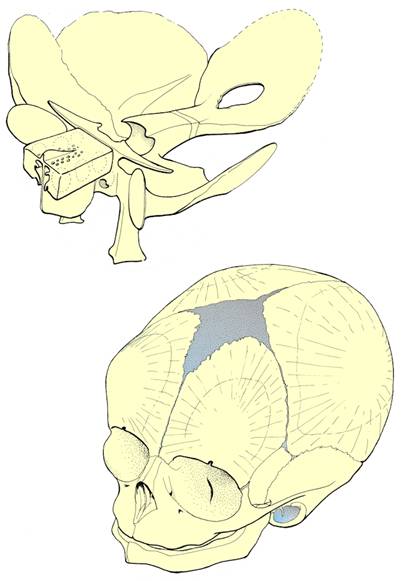
Developing fetal skull
Questions on development of the face and palate:
List the ‘building blocks' from which the face develops.
Describe the changes in position of the eyes and ears in relation to other facial structures during facial development.
Relate the nerve supply of the upper lip to its embryonic development.
How does the lacrimal duct develop?
Why are tongue movements important during palatal development? Can you think why a baby with anencephalus might also have a cleft plate?
How can a feeding bottle be modified to help a baby with cleft palate to feed?
Describe development of the nose and nasal cavities. Do the nasal cavities develop normally in a baby with cyclopia?
When do the paranasal air sinuses develop?
What is macrostomia?
