Urogenital system? You will notice that there is a considerable overlap in the development of the urinary and reproductive systems. This is particularly obvious in the male, where structures originally formed with a urinary function are 'taken over' by the reproductive system at a later stage. For example, the mesonephric duct, which at one stage drains dilute urine from the mesonephros, becomes modified to form the epididymis and ductus deferens linking the testis with the ejaculatory duct. Also in the male, the urethra becomes the final common pathway for urine and semen. Thus, it is not uncommon to see or hear references to the 'urogenital system'. The source of most of the urinary structures is the column of intermediate mesoderm, which lies between the somites (situated more medially) and the lateral mesoderm which is split into two layers by the intra-embryonic coelom. Evolutionary sequence Three 'urinary systems' appear in sequence during embryonic development, perhaps indicating the evolutionary sequence by which the definitive kidneys arose: pronephros → mesonephros → metanephros They are sequential systems in terms of:  | time of appearance: pronephros first, mesonephros next, and metanephros last | | position within the embryo: pronephros in the cervical region, mesonephros in the abdominal region, and metanephros in the pelvic region |
In the human embryo, the metanephros forms the definitive kidneys, but in other animals one of the earlier systems may be retained. 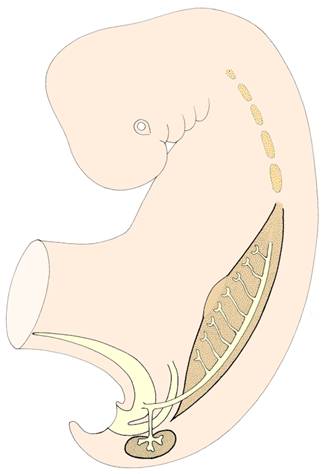
Pronephros, mesonephros, and metanephros
arising in cranio-caudal sequence. 
pronephros - vestigial In the human embryo, the pronephros regresses soon after its formation, and is probably non-functional. mesonephros – probably probably functional The mesonephros is known to be functional in embryos of some mammalian species (eg: cat, rabbit, pig), and there is reason to expect this to be the case in the human embryo too. The mesonephros develops in the posterior wall of the abdomen, and forms a pair of elongated ridges, one on each side of the dorsal mesentery. A segmental series of excretory tubules develops within each ridge and link up with a collecting duct - the mesonephric duct. The mesonephric duct drains into the allantois close to the cloaca. The excretory units - mesonephric tubules - arise in a cranio-caudal sequence, and as the more caudal ones appear, the normal cranial ones gradually degenerate and disappear. The mesonephros reaches its maximum development in week 6, after which it begins to involute. (If the embryo is male, a small number of mesonephric tubules will be retained and incorporated into the reproductive system, as you will see later.) Recall that a fold of tissues arises from the cranial end of the mesonephric ridge on each side and contributes to development of the diaphragm - these are the pleuroperitoneal membranes. metanephros - definitive kidneys As the mesonephros regresses, the definitive kidneys (ie: the kidneys seen postnatally) begin their development from the metanephros. Two important components are required to produce each kidney: | the metanephric blastema (intermediate mesoderm) | | the ureteric bud (an outgrowth from the mesonephric duct). |
The metanephric blastema differentiates into the functional units of the kidneys - the nephrons (approximately 1-2 million per kidney). However, it can only achieve this under the inductive influence of the ureteric bud. From the ureteric bud develops the collecting duct system, including the collecting tubules which link with the nephrons), the major and minor calyces, the renal pelvis, and the ureter. ‘ascent’ of the kidneys Each metanephric kidney 'ascends' from the pelvic region, where it originates, to its final position on the posterior wall of the abdomen. It seems that much of this ascent is the result of differential growth - the posterior wall of the abdomen grows rapidly so that in a sense the caudal end of the embryo 'grows away' from the kidneys. The arterial supply of each kidney changes during this ascent, with new branches being formed from the aorta at successively higher levels. Occasionally, arteries from lower levels are retained as supernumerary renal arteries. As the kidneys ascend, they have to pass beneath an arch formed by the two umbilical arteries as they course ventrally from the paired dorsal aortae to the umbilical region. This brings the kidneys close together, and occasionally their lower poles become fused forming an abnormal, U-shaped horseshoe kidney. Note that while the kidneys are ascending, the gonads are descending - their relationships become reversed! The remaining parts of the urinary system are: | the urinary bladder | | the urethra |
Their development will be considered next. urinary bladder The allantois acts as a temporary bladder, but then the definitive bladder is formed as the urorectal septum grows caudally to meet the cloacal membrane. This septum subdivides the urogenital sinus from the hindgut, and it is the 'upper' part of this sinus which differentiates into the urinary bladder. Although most of the allantois eventually regresses, it probably contributes to the apical region of the definitive bladder. Note how the ureters - initially outgrowths from the mesonephric ducts - eventually gain their own entrances into the bladder. urethra The lower portion of the urogenital sinus - between the developing bladder and the urigenital membrane - forms the urethra: all of the urethra in female embryos, but only the proximal portion in the male embryos (the distal portion is formed during development of the external genitalia, as we shall see later). Onset of function - metanephros The metanephric kidneys are functional by the beginning of the second half of pregnancy. The copious dilute urine (containing a little urea and urid acid) is released into the amniotic fluid that surrounds the fetus. However, the quantity of fluid in the amniotic cavity is regulated by an ingenious mechanism. This mechanism also rehearses the functioning of the digestive system and allows the reuptake of urea so that it can be disposed of eventually across the placental membrane. The feturs swallows amniotic fluid periodically, and the fluid is then re-absorbed from the digstive system into the fetal circulation. You may remember from our study of the developing digestive system that the debris in the fluid is acted upon by the digestive enzymes. Significant abnormalities | pelvic kidney | | horseshoe kidney | | cystic kidney | | agenesis of one or both kidneys | | duplication of the ureter | | bladder defects |
Questions on the urinary system: Is there any significance in the close relationship between the intermediate mesoderm and the intra-embryonic coelom? What happens to the metanephric blastema if the ureteric bud of that side fails to reach it? What is the embryological explanation of cystic kidney? Why is the horseshoe kidney generally positioned lower in the abdomen than normal kidneys would be? In what way is the development of the trigone different from other parts of the urinary bladder? How are the major and minor calyces of the kidney formed? What is a urachal fistula? What is the embryological explanation of exstrophy of the bladder? What clinical problems might be associated with duplication of the ureter?
| 